Haemoglobin
Haemoglobin and Disease
Decreased levels of haemoglobin, with or without the concomitant decrease in red blood cells, can cause anaemia. Iron deficiency is one cause of anaemia, as it directly affects the ability to produce haem molecules, but there are several other causes of anaemia. There can also be other disease profiles associated with abnormalities in haemoglobin, known generally as haemoglobinopathies, as well as abnormalities affecting the production of haem molecules, known as porphyrias. A few examples are described below:
Sickle Cell Anaemia
|
|
|
|
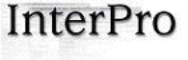
A sickle cell next to
regular red blood cells |
|

Sickle Cell Anaemia affects the shape of red blood cells, changing them from a flattened disc to a sickle or crescent shape. Whereas normal red blood cells are smooth and move easily through blood vessels, sickle blood cells are hard, inflexible and tend to clump together, causing them to get stuck in blood vessels as blood clots, thereby blocking the flow of blood. This can cause pain, blood vessel damage and a low red blood cell count (anaemia) due to the more fragile nature of sickle blood cells. The abnormal sickle shape is due to the presence of abnormal haemoglobin (haemoglobin S), which contains abnormal beta polypeptide with a single amino acid substitution at position 6 along the polypeptide chain (the alpha chain is normal). The abnormal b chain reduces the amount of oxygen inside the red blood cell, altering its shape.
Heterozygotes, where one beta chain gene is affected and the other is normal, usually display normal red blood cells, and it is only when both beta chain genes are affected (homozygote) that the sickle cell disease is seen. However, heterozygote carriers of the disease are better protected against malaria than people with two normal beta chain genes. This malarial protection has caused the sickle cell gene to reach high levels in indigenous populations in Africa and India.
Thalassaemia
Thalassaemia is caused when the production of haemoglobin chains is impaired, the most common forms affecting the alpha globin chain (alpha Thalassaemia) or the beta globin chain (beta Thalassaemia). The chains themselves can be normal, but the amounts produced are not; sometimes the genes can even be missing. There are four genes needed to make the alpha globin chain, with moderate to severe anaemia resulting when more than two genes are affected. With the beta globin chain there are two genes required, the most severe form of the disease affecting both genes. An equal number of alpha and beta globin proteins are required to make functional adult haemoglobin, and a deficiency in either chain will cause an imbalance that damages and destroys red blood cells, thereby producing anaemia. The deficiency in globin chains can cause the an abnormal association of globin chains: in the case of alpha Thalassaemia, beta globin chains combine to produce abnormal beta tetramers that cannot bind oxygen, whereas with beta Thalassaemia no such alpha tetramers exist – instead the alpha globin chains become degraded in the absence of beta globin chains.
Porphyria
Porphyria disorders affect the production of functional haem molecules in haemoglobin. The haem component is composed of a porphyrin ring complex and iron. Porphyria affects the production of a functional porphyrin complex through a genetic mutation at any one of the many enzymatic steps involved in its production. While most haem is in the blood associated with haemoglobin, haem is also required for in several other tissues, including the liver. Porphyrias can affect either the skin (cutaneous porphyria) or the nervous system (acute porphyria). Cutaneous porphyria causes the development of blisters, itching and swelling upon exposure to light, while acute porphyria causes pain, numbness, paralysis or mental disorders.
Certain light-sensitive drugs have been developed based on the abnormal porphyrin structures that result from cutaneous porphyria. These drugs have been used to treat cancer: cancer cells preferentially absorb these porphyrin-like structures and help to destroy the cancer cells upon exposure to light treatment involving lasers.
Carbon Monoxide Poisoning
Carbon monoxide (CO) binds to haemoglobin with a higher affinity (200x greater) than oxygen, and at the same binding site. Consequently, carbon monoxide will bind haemoglobin preferentially over oxygen when both are present in the lungs - even small amounts of carbon monoxide can dramatically reduce the ability of haemoglobin to transport oxygen. Levels as low as 0.02% carbon monoxide can cause headaches and nausea, while a concentration of 0.1% can lead to unconsciousness. This accounts for the suffocation caused by carbon monoxide fumes, such as from the exhaust of a car engine. People who smoke heavily can block up to 20% of the oxygen binding sites in haemoglobin with carbon monoxide. When carbon monoxide binds to haemoglobin it becomes a very bright cherry red (carboxyhaemoglobin), giving the person the appearance of a ‘healthy glow’.
By contrast, carbon dioxide (CO2), which is produced as a waste product after aerobic respiration, binds to haemoglobin at a different site, therefore does not compete with oxygen for binding to haemoglobin.